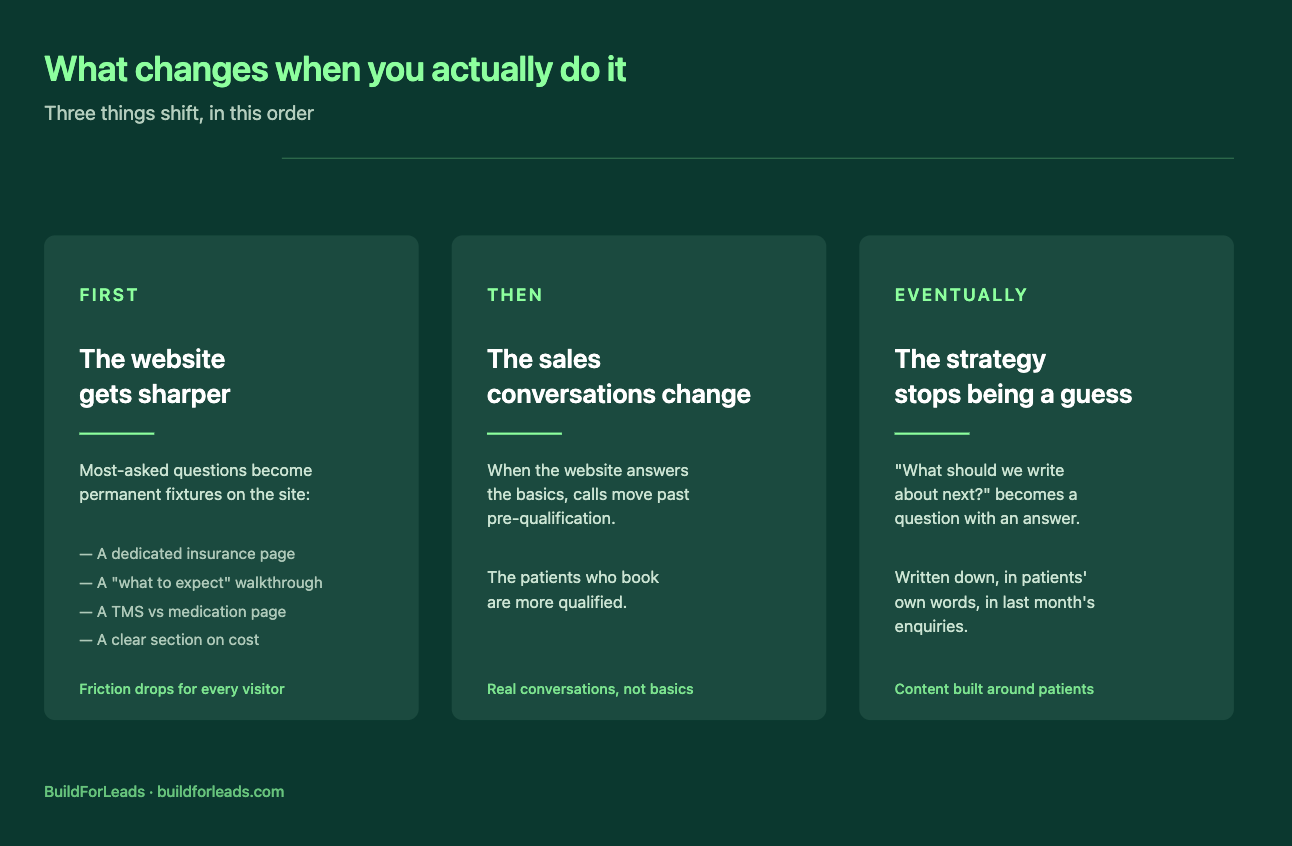

You're spending real money on ads. Patients are filling out the form on your website. The enquiries are coming in. Then the front desk picks up the phone, runs through the same questions for the tenth time that week, and discovers the person on the other end is sixteen, or hasn't tried any antidepressants yet, or is currently being treated by their existing psychiatrist and just wanted to ask a question. That's not a clinic problem. That's a form problem. A generic "contact us" form is doing the only job it knows how to do - collect a name, email, and phone number and send them through. It can't tell the difference between a strong TMS candidate and someone who's not eligible. It treats all of them the same way. And that means every consult slot, every front-desk callback, and every clinician hour is being spent on a pile of leads that haven't been sorted, even though some of them are weeks away from being treated and others were never going to be your patient. The cost of that shows up everywhere. Clinicians burn time on consults that should never have been booked. Front-desk staff spend their day chasing people who don't pick up. Genuine high-fit patients wait longer for callbacks than they should, and some of them lose patience and go to a competitor before you ever speak to them. The ad spend doesn't go down. The number of patients actually starting treatment does. The fix isn't more marketing. It's a smarter intake. What a qualification survey actually does differently A qualification survey replaces the contact form on your enquiry pages with a short, structured set of questions a patient answers before any of your team sees their name. By the time the enquiry reaches your CRM, it's already sorted, tagged, safety-screened, and routed. It works because it asks the things your front desk would ask anyway - diagnosis, prior medications, age, contraindications - but it asks them up front, in a way that turns answers into actions. Strong candidates go straight to the top of the pipeline. People who need a clinician to review something get held in a separate bucket. People who aren't candidates today get a respectful response and a follow-up sequence instead of a wasted consult slot. Under-18s are always routed to a human, never auto-approved. The patient finishes the survey, sees a result that matches their situation, and gets an email and a next step within seconds - at 2am, 11pm Sunday, or in the middle of a Tuesday afternoon.
Quick answer: Most TMS clinics under-follow-up. The ones that over-follow-up sound desperate. Both lose the same patient. Good follow-up isn't more messages - it's better ones: short, spaced properly, useful on their own, and structured to give the patient a graceful reason to re-engage instead of pressure to respond. Stop the sequence at four to six touches over three weeks. After that, keep the lead in a slower nurture, not an active chase. An enquiry comes in. The clinic calls back. The patient doesn't answer. A voicemail gets left. An email goes out. Then silence. Two days later, another call. Voicemail. Another email. Same day. Three days after that, a third message. This one says "just checking in!" with a lot of exclamation marks. By the time the patient sees any of it, they've spoken to a competitor, booked with someone else, or decided the whole thing is too complicated. The clinic that spent real ad money to generate the enquiry has now spent real staff time chasing the patient away. Most TMS clinics have this problem, and it's not one anyone gets trained on. Follow-up is where marketing hands off to operations, and neither team owns it properly. So it defaults to a mix of "try harder" and "hope for the best" - which is why most sequences end up either too quiet or too pushy, and often both in the same week. Here's what appropriate follow-up actually looks like for a TMS practice, and why the current version isn't working. Why most follow-up feels desperate The problem isn't the number of messages. It's what they say. A follow-up that sounds desperate has a specific pattern. It's about the clinic, not the patient. "Just checking in." "Wanted to make sure you got our last email." "Following up on your enquiry." All of these communicate the same thing: we haven't heard back and we're wondering why. That's the clinic's problem, not the patient's, and the patient can feel it. The tone gets more pointed when the intervals compress. Three messages in five days reads as pressure. Three messages spread over three weeks, each with something genuinely useful in it, reads as attentive care. The mistake most clinics make is assuming the answer is more touchpoints. It isn't. The answer is better touchpoints, spaced properly, that give the patient a reason to engage on their terms rather than a reminder that the clinic is waiting.
Quick answer: Most interventional psychiatry clinics run marketing in pieces — a website agency that doesn't touch the CRM, a paid team that doesn't see the intake, an SEO contractor who doesn't read a single patient survey. For Optimum Wellness & TMS in Columbus, Ohio, we rebuilt the entire acquisition system as one integrated stack: website, qualification funnel, HIPAA-compliant CRM, source-attributed call tracking, automated nurture, compliance layer, and content. One team, one system, one accountable owner from ad click to booked patient. This is what actually got built. Most TMS practice owners can describe their marketing setup the same way. A website someone built a few years ago. An intake team handling calls. Google Business Profile set up. Maybe some SEO. Maybe some ads. Different people, different pieces. Ask the same practice owner where their patients are actually coming from, and the answers get less confident. That was Optimum Wellness & TMS in Columbus when they came to us. A working website, but no call tracking, no qualification funnel, no CRM, scattered citation data, intake handled externally, and no way to see which marketing spend was actually producing patients. The marketing wasn't broken - it was invisible. Here's what we rebuilt. The website: 25 pages built around patient intent We rebuilt the Optimum site on Duda from the ground up. Service pages for TMS, Spravato, IV Ketamine, TMS for Teens, Accelerated TMS, and BrainAge. Condition pages, learning resources, a Meet the Doctor page, a Refer a Patient page, and an insurance and pricing quiz. Every service page follows the same structure: what the treatment is, who it's for and who it isn't, what a first visit looks like, how insurance and cost work, and a clear next step. Written in language patients use. The Meet the Doctor page carries more weight for TMS than most sites give it. Patients making a decision about interventional psychiatry want to see who's actually treating them. Most TMS sites bury this. We put it forward. Two landing pages built for paid traffic Two dedicated landing pages sit alongside the main site - one for TMS and Accelerated TMS, one for Spravato and IV Ketamine. Same visual system, no navigation, structured around the specific decision the ad campaign is asking the visitor to make. Both route directly to the qualification funnel. The qualification funnel: 11 slides, five outcomes At the center of the system is a structured funnel that replaces the generic contact form on every enquiry surface. Eleven short questions covering diagnosis, medication history, age (gated against FDA-cleared scope), treatment interest, treatment-specific safety contraindications, and a few free-text questions surfacing what the patient actually wants from care. At the end, the patient is routed to one of five outcome pages: strong candidate, safety review, nurture, needs follow-up, or not a fit. Each outcome triggers a different next step - automated where it can be, human-led where it needs clinical judgment. Under-18s are always routed to a person, never auto-approved. The point isn't to filter patients out. It's to make sure the intake team isn't cold-calling anonymous form submissions. When a call happens, they already have the patient's diagnosis, medication history, treatment interest, and safety flags in front of them.
Quick answer: For most healthcare clinics, the right structure isn't strictly in-house or strictly agency - it's whichever option can own the full marketing stack rather than just one piece of it. An in-house hire works well for brand, social, and internal coordination but rarely covers the technical layer (website, ads, SEO, CRM) alone. An agency works well when it owns the whole stack as one team, but most agencies own only a fragment. The decision worth making isn't between the two labels - it's which option can cover what you actually need built. At some point, every growing healthcare clinic has the same conversation. The patient numbers are good. Marketing is starting to matter more. The website needs work, the SEO isn't where it should be, the ads aren't being managed properly, and someone keeps saying "we should be doing more on social." So the question comes up at a leadership meeting: do we hire someone in-house, or do we work with an agency? It's the wrong question. The right question is what you actually need built, and whether what you're hiring can build it. Most clinics don't need "a marketer." They need a website that converts, ads that don't waste money, content that gets found, and a CRM that actually works — all running together. Whether that comes from a person on your payroll or an outside team isn't the real decision. The real decision is whether the thing you're hiring can do all of it, or only some of it. Here's what that looks like in practice. What the in-house hire actually gives you The case for hiring in-house is closeness. Someone in the building who knows your services, your team, your patients, and your culture. Communication is fast. Priorities can shift in a Slack message. The institutional knowledge stays in the clinic, not in a contract. That's real, and it matters. If you're a clinic with strong existing patient flow that needs a coordinator for social media, day-to-day communication, internal marketing oversight, and brand voice, an in-house hire is probably the right answer. Where it stops working is the technical layer. Modern healthcare marketing requires SEO, paid advertising, website development, conversion optimization, analytics, and increasingly CRM and intake automation. Expecting one person to cover all of that — at the level a competitive market demands — isn't realistic. The clinics that try usually end up with a coordinator doing what they can across too many areas, while the technical work either doesn't happen or gets contracted out anyway. The honest version of in-house marketing is: it works well for the relationship layer, less well for the technical layer, and the technical layer is where most clinics lose patients. What an agency actually gives you - and what most don't The case for working with an agency is access to specialists across multiple disciplines without having to build a department. That's the pitch. In practice, most agencies deliver less than that promise suggests. The web agency doesn't touch the ads. The SEO contractor doesn't talk to the PPC team. The CRM is somebody else's problem. The clinic ends up paying multiple vendors, none of whom are accountable for whether the system as a whole is producing patients. The structural problem with most agencies isn't expertise - it's fragmentation. When the website team can't see the ads data, when the ads team can't change the landing page, when the CRM lives outside the picture entirely, the marketing operates in disconnected pieces. The patient lands somewhere, falls through a gap, and nobody is the right person to fix it. The agencies worth working with are the ones who built around that problem from the start - where the team that touches your website also touches your content, your ads, your CRM, your intake. One team. One contract. One accountable owner for the whole funnel. That's the difference worth paying for. Not "an agency" in the abstract. An agency that owns the stack.
Most TMS clinics spend their marketing energy on the first half of the problem - getting found. SEO, Google Ads, local listings, AI search visibility. All of it is built around the same goal: showing up when a patient searches. Then the patient lands on the website, looks around for ninety seconds, and leaves. Showing up is the table stakes. It's not the conversion. Between a patient finding your clinic and a patient picking up the phone, there's a trust layer most TMS websites skip past - and that's where the consults are quietly being lost. Here's what patients are actually looking for in those ninety seconds, and why most clinic sites don't give it to them.

Customers are no longer starting on Google. A growing share of them open ChatGPT, Perplexity, or Google's AI Overviews, type a question - "best [your service] near me," "who should I use for X," "what's the best [product] for [situation]" - and read the answer. Two or three businesses get named. The rest are invisible. That invisibility is the unsettling part. When you lose a Google ranking, you see it happen in your analytics. When an AI tool recommends your competitor to a thousand potential customers, nothing shows up in any report you currently run. Ranking well on Google does not mean you'll be cited by AI. Research suggests the overlap between top Google results and AI-cited sources is shrinking fast. You can be the number-one organic result and still never get mentioned in the answer. The first step isn't to fix it. It's to find out where you stand. Here's how to do that in under an hour.
Most TMS clinics spend their marketing budget getting patients to enquire. The website, the SEO, the ads - all of it exists to turn a stranger into someone who picks up the phone or fills in a form. Then the enquiry comes in, and the system that worked so hard to create it quietly drops the ball. This is the part of patient acquisition almost no clinic measures, and it's where a lot of expensive marketing goes to die. You can have the best website in your market and still lose the patient in the gap between "I'm interested" and "I've booked." Here's how that gap opens up, and what closing it actually looks like. The patient isn't waiting for you. They're comparing you. When someone enquires about TMS, they are rarely enquiring with one clinic. They're anxious, they've usually exhausted other treatment options, and they're doing what anyone does with a high-stakes decision - looking at several providers at once. That changes everything about what happens next. The patient who fills in your form at 2pm isn't sitting by the phone hoping you call back. They've also messaged the clinic across town, and maybe a third. Whoever responds first, clearly, and warmly is the one who gets the conversation. The others are competing for a patient who's already half-committed elsewhere. The research on this is consistent across industries: the large majority of customers end up going with whoever responds first - not the cheapest, not the most credentialed, but the first. For a TMS clinic, that means the quality of your care is irrelevant to the patient who never heard back in time to consider it. Speed is the variable nobody is managing The uncomfortable truth is that most clinics have no idea how fast they respond to enquiries, because nobody owns the number. A form comes in. It lands in an inbox that someone checks between patients. A voicemail sits until the front desk has a quiet moment. An after-hours enquiry waits until the next morning - by which point the patient has already spoken to someone else. None of this is negligence. It's just what happens when enquiry response is everybody's job and therefore nobody's job. The marketing generated the lead; the clinical team is busy treating patients; the front desk is managing a waiting room. The enquiry falls into the space between them. The clinics that convert well aren't working harder. They've simply decided that responding to an enquiry is a defined job with a defined target - minutes, not hours - and built a small amount of process around making that happen reliably. After-hours is where the most patients are lost Here's the part that's easy to miss. A meaningful share of TMS enquiries arrive outside clinic hours - evenings, weekends, the moments when someone finally sits down, opens their laptop, and decides to do something about how they've been feeling. That timing is not a coincidence. It's often when the patient is most motivated. And it's exactly when most clinics are least equipped to respond. If your only response mechanism is a person checking an inbox during business hours, every evening and weekend enquiry cools for twelve hours or more before anyone touches it. By Monday morning, the patient who enquired on Friday night has had a whole weekend to talk to a competitor, change their mind, or lose the nerve it took to reach out in the first place. This is the single biggest fixable leak in most clinics' patient acquisition, and it has nothing to do with the website..

Choosing a marketing partner is one of the more expensive decisions a healthcare clinic will make, and one of the easier ones to get wrong. Most agencies tell you the same things. More traffic, better SEO, more patients. The pitches are interchangeable, the case studies sound similar, and the monthly fees are often comparable. The differences only become clear six months in - after the contract is signed and the budget is spent. Here's what actually separates a good agency from the right one. Does the agency understand healthcare specifically? Healthcare marketing is not the same as marketing retail or e-commerce. Patients searching for care are anxious, often researching during difficult moments, and weighing decisions with real consequences. The messaging that works for a furniture brand does not transfer. A healthcare-experienced agency understands: Patient decision-making and the emotional weight behind clinical searches Compliance constraints around medical advertising The trust signals that matter on a clinic website How to write about conditions and treatments without crossing clinical or legal lines A generalist agency will treat your clinic like any other client . That usually shows. Worth asking: how many healthcare clients have you worked with in the past two years, and what types of clinics? Are they leading with strategy or tactics? A lot of agencies open with a deliverable. A new website. An SEO package. A monthly ad spend. The tactics are real, but they're being offered before anyone has asked what your clinic actually needs. A strong marketing partner starts with strategy. They want to understand your growth goals, your current patient pipeline, your geographic reach, and where the competitive pressure is. Those answers decide whether you should prioritise local SEO, paid search, landing pages, content, or some combination. Without that foundation, the marketing becomes reactive - a series of tactics chosen because they're what the agency happens to sell. Worth asking: how would you approach our clinic in the first 30 days, and what would you want to understand before recommending anything? How transparent is the reporting? A marketing partnership should not feel like a black box. Every month, you should know: What work was done and why Which objectives it was tied to How is performance being measured What's being adjusted based on the data If the monthly update is a dashboard of impressions and clicks with no narrative and no link to patient enquiries, you are paying for activity rather than outcomes. Worth asking: can I see a sample of the monthly reporting you provide to clients?

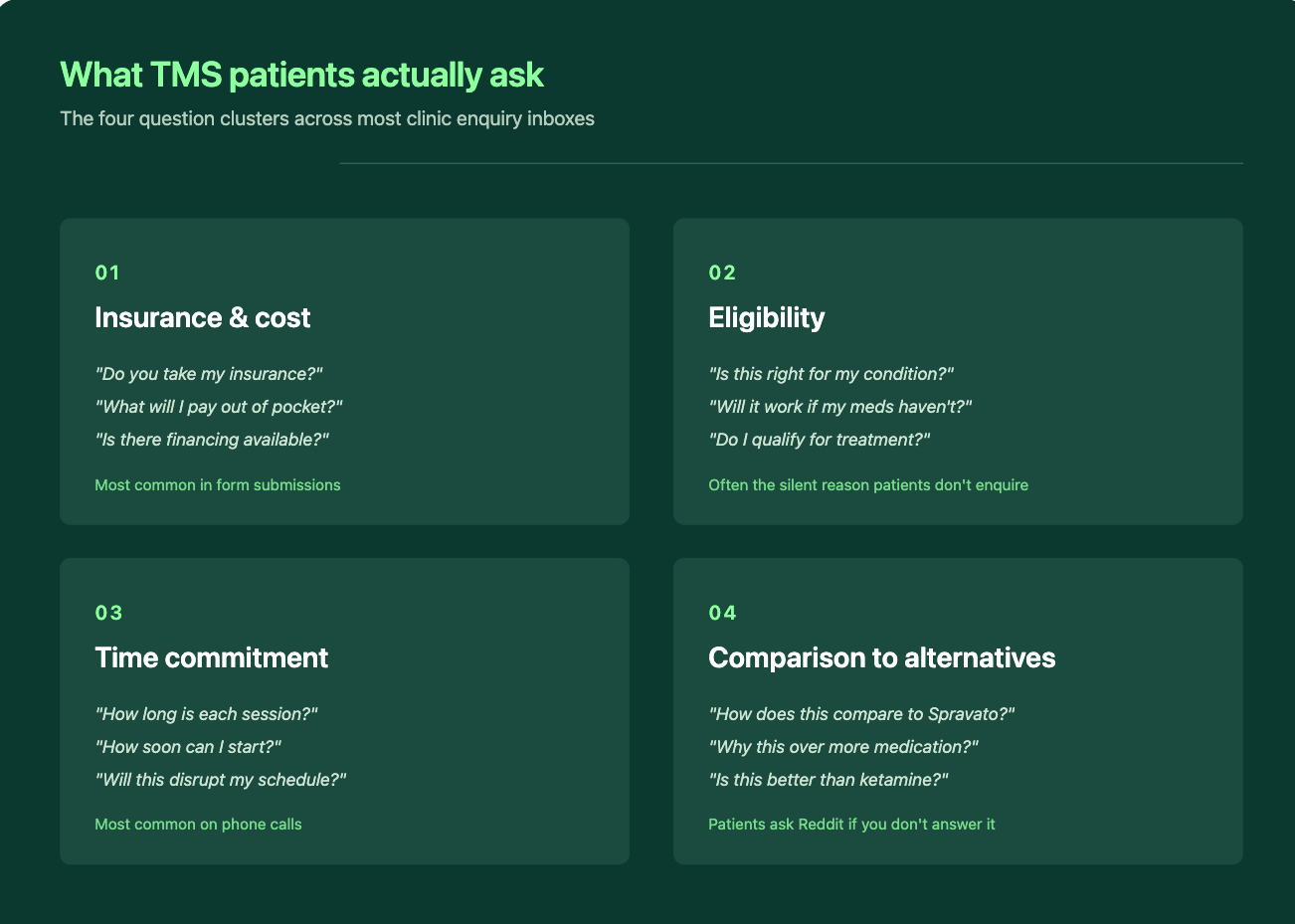
For a clinic offering more than one interventional psychiatry treatment, the patient on your website isn't asking "should I try TMS?" - they're asking "which of these is right for me?" That second question is harder. It's also the one most clinic websites quietly fail to answer. This post is about the cross-treatment decision logic patients are actually running through when they land on your site — and what a website built for that decision looks like in practice. What are patients comparing when they land on your site A patient researching interventional psychiatry rarely arrives knowing which treatment they want. They arrive somewhere along this spectrum: They've tried two or three medications, none of which have worked well, and a friend or their psychiatrist mentioned "you should look into TMS or Spravato" They've read about ketamine therapy somewhere and want to know if it's the same as Spravato (it's not, quite) They've heard about accelerated TMS or SAINT and want to know if that's faster than the standard protocol They've seen Spravato advertised, called their insurance, and are now confused about whether they qualify The thing every one of those patients has in common: they're comparing treatments before they're comparing clinics. A typical example: a clinic offers TMS, Spravato, and IV ketamine. The website has three service pages, three different contact forms, and a single "Book a Consultation" CTA across all of them. A patient with treatment-resistant depression lands on the homepage, doesn't know which of the three applies to her, opens all three service pages in separate tabs, and leaves twenty minutes later more confused than when she arrived. None of the three pages helped her choose. That's the gap. If your website only presents TMS, Spravato, and IV ketamine as three separate service pages with their own CTAs, the patient still has to do the comparison work themselves. Most won't. They'll leave, go to Reddit or WebMD, and come back to a different clinic that helped them choose. The three decisions patients are actually making Each cross-treatment comparison comes down to a specific set of questions. Clinic websites that convert well address each one directly. TMS vs antidepressant medication Most patients arriving at an interventional psychiatry clinic have been on medication for a while and aren't getting the response they hoped for. They want to know: Is TMS a replacement for my medication, or do I stay on it? How is the effect different from a new pill? Will the relief last after the six-week course ends? What does the day-to-day actually look like compared to taking a pill? Most TMS service pages explain the neurological mechanism. Almost none explain what the patient should expect compared to their current medication. That gap is where the inquiry is lost. Spravato vs IV ketamine This is the comparison most likely to be searched and least likely to be answered well on clinic websites. The two treatments are pharmacologically related but operationally very different: Spravato is FDA-cleared for treatment-resistant depression, administered in-clinic as a nasal spray, observed for two hours after each dose, and covered by most commercial and government insurance plans with prior authorization. IV ketamine is administered as an infusion, typically over 40 minutes, and is almost always cash-pay because most insurance plans don't cover off-label ketamine infusions for depression.
The short answer is yes. The longer, more useful answer is that the question is the wrong question. The clinics' ranking for searches like "accelerated TMS cost" has already moved on from that debate - their pricing is on the page. The question they're asking is harder: How do you publish pricing when fees vary by insurance, protocol, income, and whether the patient prepays? That's what this post is about. Not whether to publish - that ship has sailed - but how to do it without losing insurance-paying patients or painting yourself into a corner you can't update later. Why "we work with most major insurers" doesn't count Most TMS clinic websites have something that gestures vaguely at pricing. "We accept most major insurers." "Contact us for a personalised quote." "Costs vary depending on your treatment plan." That's not transparency. It's hedging dressed up as helpfulness. A patient searching "how much does TMS cost" doesn't need to be told that costs vary. They know that. They want a number (any number) to anchor their thinking against. Without one, they leave and find a clinic that gives them one. Increasingly, that's also what Google rewards. Search any high-intent TMS cost query, and the top organic results are clinics publishing real figures. The clinics still hedging are nowhere on the first page.